
LOOKS LIKE A MIRACLE TO ME!
ALL THE NEWS THAT FITS IN PRINT THAT LOOKS TOO GOOD TO BE TRUE!

Click to add an engaging title. High quality images go a long way in looking professional online.
IT'S A MIRACLE!!!!!!
(...well sort of.....)
I apologize if this has been addressed already, I'm not 100% sure where I first saw this article, may have been FB may have been a random news site. Before a lot of excitement and chatter gets cranked up about it, I thought I'd do some deep diving and see what I could find. What I found is VERY promising....for Osteoperosis patients....for folks with OI, not so much.
Any time I talk in absolutes I get hate bombs so I will say it this way:
In most reported cases of OI in North America the core issue underlying your case of OI and what tends to make your bones weak is a collagen related problem
In some cases your body cranks away day and night creating precisely the right amount of collagen your body needs...its just not of very good quality..
Then there are situations where by your body does what it can to create decent quality collagen, but there's not nearly enough of it.
Both lead to more fragile skeleton, but for radically different reasons. I will use an image from the original article for demonstration purposes, but this is one of the cleanest looking images to show what I mean that I've seen in a long time:
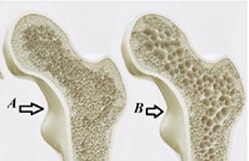
We will call Bone A from a quality OI patient, his body produces enough collagen just not very good quality collagen. Which leaves us with Bone B as being the patient who produces OK quality just not nearly enough. From an 8th grade biology perspective it almost makes sense that this solution of affecting the GPR133 may not do much for Bone A. but just looking at it, it does seem as though its going to help , in some way, “fill in the spaces” left in Bone B. While if those spaces were created by a lack of osteoblasts then it should, following the science published thus far, fill in the blanks, but as we know OI is more abut Collagen than it is about bones. Broken Bones is how the issue most commonly displays itself to the outside world.
he Direct Connection: Shared Bone Biology
No published study to date has identified GPR133 mutations as a related cause of osteogenesis imperfecta (OI), thus far most medical researchers agree that OI is a genetic issue involving COL1A1 and CO1A2, effecting collagen mutations. However, the mechanistic overlap is substantial and could be scientifically meaningful.
Genome-wide association studies (GWAS) in humans have linked gene variants of GPR133/ADGRD1 to variations in bone mineral density and body height  ScienceOpen — two of the core features also affected in OI, demonstrating a “near miss” cross section. Notably, the same paper explicitly draws a conceptual bridge, noting that low bone mass and strength lead to fragility fractures in both elderly individuals with osteoporosis and children with osteogenesis imperfecta. ScienceOpen.
ScienceOpen — two of the core features also affected in OI, demonstrating a “near miss” cross section. Notably, the same paper explicitly draws a conceptual bridge, noting that low bone mass and strength lead to fragility fractures in both elderly individuals with osteoporosis and children with osteogenesis imperfecta. ScienceOpen.
Constitutive Gpr133/Adgrd1-deficient mice exhibit reduced bone volume and strength. A lower number of osteoblasts and a reduced bone-formation rate suggest a specific role for GPR133/ADGRD1 in osteoblast function. PubMed Central This mirrors the osteoblast dysfunction that is central to OI pathophysiology.
This osteopenic phenotype in receptor-deficient mice is caused by impaired osteoblast function, which in turn promotes increased osteoclast activity. Nature The uncoupling of bone formation and resorption is a well-recognized feature of OI as well.
GPR133/ADGRD1 regulates osteoblast function and differentiation through a combined activation mechanism involving interaction with its endogenous ligand PTK7 and mechanical forces. GPR133/ADGRD1-mediated osteoblast differentiation is driven by cAMP-dependent activation of the β-catenin signaling pathway. PubMed Central WNT/β-catenin signaling is a well-established regulator of bone mass and has been implicated in OI-related pathways.
Activation of GPR133/ADGRD1 with the receptor-specific ligand AP-503 enhances osteoblast function and differentiation, both in vitro and in vivo, significantly alleviating osteoporosis in a mouse ovariectomy model. These findings position GPR133/ADGRD1 as a promising therapeutic target for osteoporosis and other diseases characterized by reduced bone mass. PubMed Central
A second line of research found that a small molecule agonist called GL64 negatively regulates bone loss by inhibiting osteoclastogenesis via the cAMP-PKA-NFATC1 pathway, and prevented bone loss in an osteoporosis mouse model. Science
Feature
GPR133 Deficiency
Osteogenesis Imperfecta
Reduced bone mineral density
✅
✅
Impaired osteoblast function
✅
✅
Increased osteoclast activity
✅
✅
Bone fragility / fractures
✅
✅
WNT/β-catenin involvement
✅
✅
Bottom line: While GPR133 has not been identified as a causative gene for OI, the receptor plays a central role in the same bone remodeling machinery disrupted in OI. The research strongly suggests GPR133 agonists could be a candidate therapeutic avenue for OI, particularly in forms where osteoblast insufficiency is prominent. This is an area that warrants direct investigation. If you're following this for clinical or research purposes, watching for upcoming studies exploring GPR133 agonists in OI models would be worthwhile.